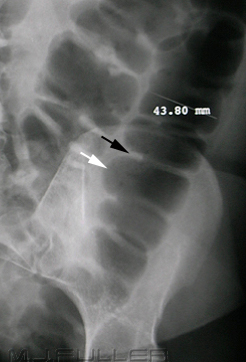
Small bowel obstruction (note the dilated loops of small bowel creating a “coiled-spring” appearance).
Large bowel obstruction
Differentiating between the small and largebowel on an abdominal X-ray is not always straightforward but there are a number of clues that may help you:
The small bowel usually lies more centrally, with the large bowel framing it.
The small bowel’s mucosal folds are known as valvulae conniventes and are visible across the full width of the bowel.
The large bowel wall features pouches or sacculations that protrude into the lumen, known as haustra. In between the haustra are spaces known as plicae semilunaris. The haustra are thicker than the valvulae conniventes of the small bowel and typically do not appear to completely traverse the bowel. This distinction is unfortunately unreliable as dilated large bowel can have a haustral pattern that does, in fact, traverse the bowel.
Faeces have a mottled appearance and are most often visible in the colon, due to trapped gas within solid faeces
The 3-6-9 rule is a simple aide-memoire describing the normal bowel caliber: